What is Harm OCD? Symptoms, Causes, and Treatment
By David Gofman, MA, LPC ·

You pick up the kitchen knife to cut up some vegetables and a thought flashes through your mind: what if I hurt someone? Or you’re driving and imagine suddenly swerving into oncoming traffic. Or you’re holding a baby and a terrible image appears, unbidden, that you would never in a thousand years choose to have.
Suddenly you feel a flood of overwhelming fear and anxiety. Why did I just think that? W_ould I actually do that? Could I? What kind of person even thinks that?_
If this is familiar, you may be dealing with harm OCD, one of the most distressing and most misunderstood subtypes of obsessive-compulsive disorder.
What Is Harm OCD?
Harm OCD is a subtype of OCD in which intrusive thoughts center on the fear of harming others — or sometimes oneself. The thoughts typically take the form of violent images, sudden impulses, or “what if” scenarios that feel deeply wrong and deeply alarming to the person experiencing them.
The defining clinical feature is that these thoughts are what’s called ego-dystonic: they are experienced as foreign, unwanted, and completely at odds with who the person is and what they value. This is what separates harm OCD from actual violent ideation. Someone with harm OCD is not someone who wants to hurt people and is fighting the urge. They are someone who is horrified by the thought and cannot stop worrying that the thought actually says something about them.
That effort to prove that they aren’t the person they fear they might be often leads to checking behaviors and reassurance-seeking, while avoidance of situations that might trigger the thoughts is often present as well.
The thoughts themselves are not the disorder. Intrusive violent thoughts are, according to research, remarkably common in the general population. In fact, studies consistently find that the majority of people who do not have a diagnosable mental disorder experience unwanted and often disturbing thoughts and mental images. What distinguishes OCD is not the presence of these thoughts but how the mind’s interpretation of the thoughts as significant or meaningful in some way, leading to intense fear, anxiety, and a compulsive response.
Harm OCD Symptoms: What It Actually Looks Like
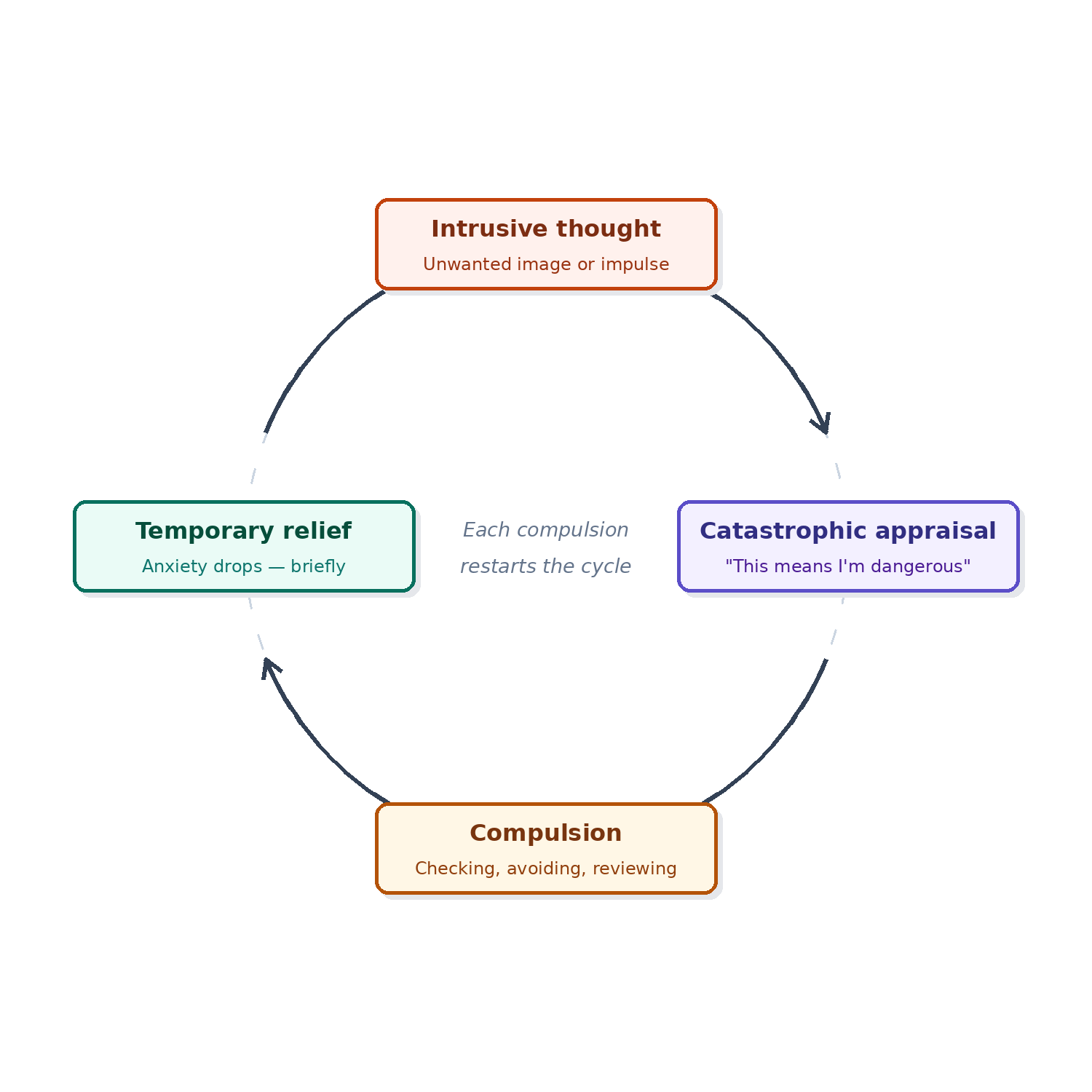
Harm OCD looks different from person to person, but the underlying structure is consistent: an intrusive thought triggers intense anxiety, which triggers a compulsion to neutralize or resolve the anxiety, which provides temporary relief, which reinforces the cycle.
The intrusive thoughts
Common harm OCD thoughts include:
- Fears of stabbing or hurting a family member
- Sudden images of violence while performing ordinary tasks
- Fears of losing control while driving
- Intrusive thoughts about harming infants or children.
The specific content often targets whatever the person cares most about — a loving parent will have thoughts about their child, a devoted partner will have thoughts about their spouse. Others may have thoughts about losing control and harming a stranger.
An important feature of Harm OCD is that the distress a person experiences is generated by the presence of the thoughts themselves. The intensity of the fear is a measure of how deeply that kind of harm violates your values, not evidence that you’re secretly capable of it.
The compulsions
Compulsions in harm OCD are often invisible to outsiders, which is part of why it’s so isolating. They typically include:
- Mental reviewing and checking — repeatedly replaying events or scenarios to confirm nothing bad happened, or that you didn’t want it to happen.
- Mental Rituals - Repeating certain thoughts or phrases, counting in specific patterns, singing a specific song in your head, or some other ritualized response to neutralize the thought or to prevent it from coming true.
- Reassurance-seeking — asking family members “I would never hurt you, right?” or searching online for confirmation that intrusive thoughts don’t make you dangerous.
- Avoidance — staying away from knives, from driving, from being alone with children, from anything that might trigger the thought or feel like an opportunity for harm.
- Thought suppression — actively trying not to think about it, which reliably makes the thought more frequent and more distressing.
- Physical compulsions may include needing to repeat certain behaviors or actions that you were doing when the harm OCD thoughts arose, either a certain number of times or until the thought goes away.
The cruel irony of these compulsions is that, no matter how logical they feel in the moment, they confirm to your nervous system that the thought needed to be taken seriously. That reinforcement is what keeps the strengthen’s your OCD.
How to tell it’s harm OCD and not something else
The question people with harm OCD most frequently ask is some version of: but what if I’m actually dangerous?
The clinical answer is that ego-dystonic thinking — thoughts that feel alien, repulsive, and threatening to your own sense of self — is fundamentally different from genuine violent ideation. People who actually intend to harm others do not typically spend their days in terror that they might. Harm OCD tends to produce the opposite of intent: avoidance, hypervigilance, and a desperate need to be certain the thought means nothing.
If you are in distress about these thoughts, that distress is clinically meaningful information. And there is good news: treatments like Exposure and Response Prevention (ERP) have been shown to be highly effective at providing long-term relief from harm OCD.
That said, this post is not a diagnosis. If you’re uncertain about what you’re experiencing, a clinical assessment with a therapist who specializes in OCD is the appropriate next step.
What Causes Harm OCD?
OCD, including harm OCD, is generally understood through three intersecting factors: biological, hereditary, and environmental.
Biological factors include dysregulation in circuits connecting the prefrontal cortex, the thalamus, and the basal ganglia — areas that play a central role in filtering signals, evaluating threat, and determining which thoughts deserve attention. In OCD, this filtering system misfires, flagging ego-dystonic intrusive thoughts as urgent and dangerous rather than allowing them to pass. Serotonin is also thought to play a role: SSRIs, which act on serotonin pathways, are among the most effective pharmacological treatments for OCD, suggesting that serotonin dysregulation is part of the picture — though the relationship is more complex than a simple chemical imbalance.
Hereditary factors are well-documented. OCD runs in families, and research consistently finds higher rates of OCD among first-degree relatives of people with the disorder than in the general population. This doesn’t mean OCD is inevitable if a parent or sibling has it — heritability estimates suggest genetics account for roughly 40–65% of the risk — but family history is one of the stronger predictive factors we have.
Environmental factors include learned responses to anxiety and distress, early experiences that shape how threat is interpreted, and major life transitions that introduce new responsibilities or stressors. Becoming a parent is a well-documented trigger, particularly for harm OCD centered on infant safety. Stress doesn’t cause OCD in someone with no underlying vulnerability, but it can activate or intensify symptoms in someone who has one.
What doesn’t cause harm OCD: a secret desire to hurt people. The content of OCD thoughts is not a window into hidden wishes. It is, if anything, an inverted map of what the person values most.
How Harm OCD Is Treated
The gold-standard treatment for harm OCD is Exposure and Response Prevention (ERP) — a specialized, evidence-based form of therapy that directly targets the obsession-compulsion cycle.
ERP works by gradually and systematically exposing the person to the thoughts, images, or situations that trigger obsessions, while supporting them in resisting the compulsive response. In harm OCD, this might involve holding a kitchen knife while tolerating the uncertainty of the intrusive thought — without reassurance-seeking, without mental checking, without avoidance. Through these experiences the brain learns that the thought is not a signal requiring a response, and the anxiety diminishes.
ERP is not about convincing you the thought is harmless. It is about changing your relationship to the uncertainty by building the capacity to have the thought without treating it as an emergency.
General CBT, mindfulness practices, and medication (SSRIs are commonly used in OCD treatment) can all play supportive roles. But ERP is the treatment with the strongest evidence base for OCD, including harm subtypes, and what most OCD specialists will recommend as the primary intervention.
One important note: generic talk therapy that focuses on exploring why you have the thoughts, or therapists who provide direct reassurance that you would never act on them, can inadvertently reinforce the compulsive cycle. If you’re seeking treatment, look for a therapist with specific ERP training and experience treating OCD subtypes.
If you’re based in Connecticut or Virginia and want to talk through what you’re experiencing, Gofman Therapy and Consulting offers ERP for OCD in Westport and virtually.
When to Consider Therapy for Harm OCD
If harm OCD is interfering with daily life — if you’re avoiding situations, losing hours to mental checking, or withdrawing from relationships out of fear — that’s a signal that self-directed reading has probably taken you as far as it can.
ERP for harm OCD is highly effective, but it’s also genuinely hard to do well on your own. The work of sitting with uncertainty, without reaching for a compulsion, benefits substantially from a therapist who knows how to pace the work and hold the discomfort with you.
At Gofman Therapy and Consulting, we offer OCD therapy and ERP treatment in-person in Westport, CT and virtually throughout Connecticut and Virginia.
David Gofman, LPC, is a therapist at Gofman Therapy and Consulting in Westport, CT. He specializes in ERP for OCD and anxiety disorders, Pain Reprocessing Therapy for chronic pain, and works with teens, young adults, and young professionals in-person and virtually across Connecticut and Virginia.


