Your relationship is good. Your partner is kind. Communication is solid. Nothing is obviously “wrong” — and that’s exactly why the doubt can feel so disorienting.
The questions keep returning anyway: Do I really love them? What if they’re not the one? What if I’m settling? You look for evidence, can’t find it, and then feel compelled to check again. You replay conversations, scan for the “right” feeling, and ask for reassurance in slightly different ways. The relationship keeps passing the test, but the doubt keeps coming back.
That pattern is common in Relationship OCD (ROCD). Relationship OCD is an OCD theme in which intrusive doubts about a relationship trigger compulsions such as reassurance seeking, checking feelings, and mental review. The loop typically doesn’t deliver new information about the relationship. It reinforces a cycle of uncertainty → anxiety → compulsions → brief relief → more doubt.
"ROCD is maintained less by the doubt itself and more by the compulsions used to neutralize uncertainty — reassurance, checking, mental review — which provide brief relief but reinforce future doubt."
— David Gofman, LPCThis article is educational and isn’t a diagnosis. If you’re struggling, a licensed clinician can help you clarify what’s going on and what treatment fits.
What is relationship OCD?
Relationship OCD (ROCD) is best understood as a content focus of OCD, not a separate diagnosis. The obsessions attach to a relationship—your feelings, your partner, the “rightness” of the match—and the compulsions are the strategies you use to try to neutralize uncertainty.
A useful clinical marker is the function of the thoughts and behaviors. In ROCD, the mind treats uncertainty as an urgent problem that must be solved immediately. Attempts to get certainty—by analyzing, checking, comparing, or seeking reassurance—tend to feel temporarily relieving and then quickly insufficient. The longer you spend trying to think your way to relief, the more “sticky” and convincing the doubt can become.
ROCD can look like “relationship anxiety,” but it tends to be more repetitive, more time-consuming, and more tied to rituals (including mental rituals). Treatment focuses less on proving whether a relationship is “right” and more on interrupting the compulsive cycle so you can tolerate uncertainty and make choices based on values rather than fear.
Relationship OCD symptoms
When people search relationship OCD symptoms, they’re usually describing two things:
intrusive doubts that feel hard to disengage from, and
a pattern of checking or reassurance that provides only short-lived relief.
Common ROCD obsessions (intrusive doubts)
ROCD obsessions often show up as “what if” questions or urgent mental debates, such as:
Do I really love them?
What if they’re not the one?
What if I’m settling or making a mistake?
What if I’m not attracted enough—and that means something?
Persistent focus on a partner’s perceived flaws, with a feeling you must resolve the concern to feel calm
Fear that uncertainty itself is proof something is wrong
Common ROCD compulsions (including mental compulsions)
Compulsions can be visible behaviors or internal “mental moves.” Both can keep the cycle going:
Reassurance seeking: asking your partner, friends, or a therapist to confirm the relationship is okay; repeated “Do you love me?” / “Are we okay?” conversations
Checking feelings: scanning your body/mood for the “right” feeling; testing attraction; monitoring whether you feel certain enough
Mental review/rumination: replaying conversations, comparing past “good moments” vs “bad moments,” building arguments for/against staying
Comparison rituals: comparing your relationship to others, to past relationships, or to an imagined ideal
Compulsive research: searching online for signs, quizzes, forums, or “proof” you’re in the right relationship
Confessing for relief: repeatedly disclosing doubts to reduce guilt or anxiety
Avoidance: pulling back from intimacy, commitment steps, or time together to avoid triggering doubt
Signs of relationship OCD vs normal relationship doubt
Most relationships include uncertainty. Signs of relationship OCD tend to involve:
Doubts are repetitive and intrusive, not occasional reflection
You feel driven to do something to reduce them (reassurance, checking, analyzing)
Relief is temporary, and the same question returns or shape-shifts
The process takes up meaningful time and affects mood, sleep, focus, or intimacy
You feel like you can’t move forward without certainty
Rule of thumb: normal doubt often responds to reflection, conversation, or time. ROCD doubt tends to demand a ritual to get relief.
The ROCD cycle (what keeps the doubt going)
ROCD is often less about the content of the doubt and more about the process you get pulled into.
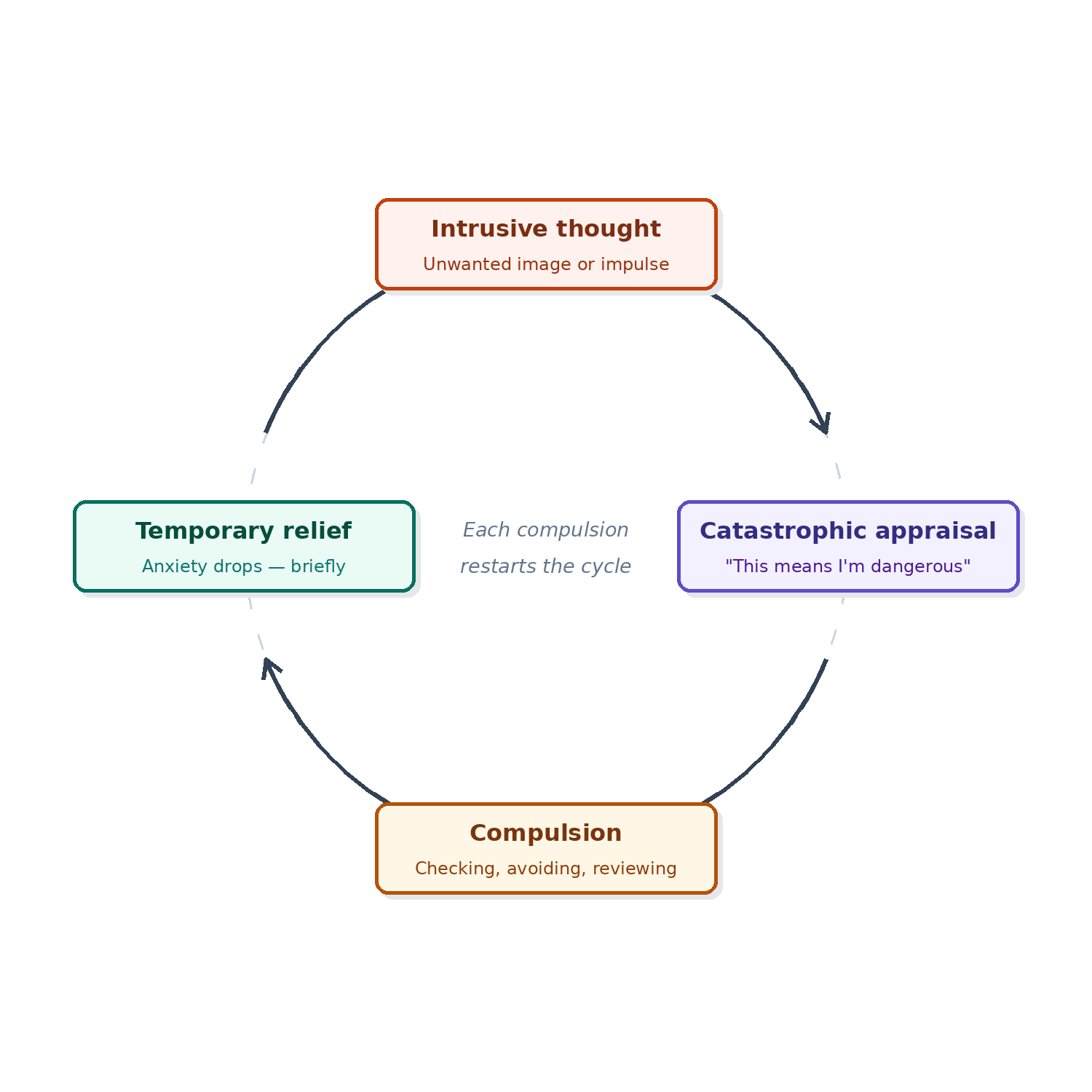
A typical ROCD cycle:
Intrusive doubt or discomfort (“What if I don’t love them enough?”)
Anxiety / urgency (“I need to know for sure”)
Compulsions (reassurance seeking, checking feelings, mental review, comparisons, researching)
Short relief (“Okay…maybe we’re fine”)
Return of doubt (often stronger, more convincing, or in a new form)
Key clinical point: compulsions reduce anxiety briefly, which teaches the brain to repeat them in order to feel better. No matter how much you think about the relationship, ROCD thoughts will always surface, causing increased distress and escalations in checking.
ROCD vs relationship anxiety vs real relationship problems
These three things can look similar from the inside, and distinguishing them matters for treatment.
Relationship anxiety is typically responsive to context. A rupture of trust increases anxiety; as trust is rebuilt, the anxiety recedes. A difficult week produces more worry; a good week produces less. Reassurance from a partner tends to help meaningfully, and the relief has some durability.
ROCD tends to be decoupled from context. The doubt doesn't reliably track what's actually happening in the relationship — it can be most intense when things are going well, and it doesn't meaningfully respond to evidence. A loving gesture, a good weekend, or a clear-headed conversation might help for an hour. Then the question returns. This is the pattern your hook describes: the relationship keeps passing the test, and it doesn't matter.
The other defining feature of ROCD is compulsions. Relationship anxiety might involve occasional reassurance-seeking or avoidance. ROCD generates systematic, driven rituals — repeated reassurance conversations, mental review, feeling-checking, online research, comparison — that follow a predictable cycle. The compulsions are what make it OCD rather than anxiety.
Real relationship problems are different from both. Genuine incompatibility, disrespect, or chronic boundary violations show up as consistent, observable patterns in behavior — not just in anxious moments. They don't shape-shift the way ROCD doubt does, and they don't disappear when you stop checking.
A useful question: does the doubt track what's actually happening in the relationship, or does it seem to have a life of its own? If evidence doesn't move the needle and compulsions are part of the picture, ROCD is likely involved.
Important: If there is emotional abuse, physical violence, coercion, or safety concerns, treat that as a separate clinical priority and seek appropriate support.
What causes relationship OCD?
People often ask what causes relationship OCD because they assume the relationship itself must be the problem. In reality, ROCD is driven by the same mechanisms that fuel OCD more generally: a strong discomfort with uncertainty and compulsions that temporarily soothe anxiety but strengthen it over time.
Common contributors include:
Intolerance of uncertainty: the urge to know “for sure”
Threat monitoring: scanning for danger signals (“Is this a red flag?”) even when evidence is limited
Over-responsibility: feeling you must prevent mistakes at all costs
Perfectionism: believing love should feel constant, clear, and conflict-free
Attachment triggers: closeness, vulnerability, fear of loss, fear of making the “wrong” choice
Reinforcement learning: reassurance and checking reduce anxiety short term, which teaches the brain to repeat them
This is why ROCD can show up in relationships that are otherwise supportive and stable.
For a fuller look at the biological, hereditary, and environmental factors that underlie OCD across subtypes, see What Is Harm OCD?
Relationship OCD treatment: what helps most
If you’re searching for relationship OCD treatment, the headline is this: the most effective treatment for OCD is typically a specialized behavioral approach called Exposure and Response Prevention (ERP).
ERP helps you practice facing triggers and uncertainty while reducing compulsions—especially reassurance seeking, checking, and rumination. Over time, the brain learns that uncertainty is uncomfortable but not dangerous, and that you don’t have to solve every doubt to live your life.
What ERP for ROCD can look like
ERP for ROCD is tailored to your patterns. Examples may include:
Learning to label intrusive doubts as OCD thoughts rather than facts
Practicing leaning into uncertainty without trying to solve it
Reducing reassurance seeking (from partner, friends, and online searching)
Reducing checking behaviors (testing attraction, scanning feelings)
Cutting down mental review and “relationship analysis sessions”
Building tolerance for uncertainty and for feelings that fluctuate (because feelings do fluctuate)
ERP isn’t about forcing yourself to stay in a relationship no matter what. It’s about stepping out of compulsive certainty-chasing so you can relate to thoughts differently and make decisions from values rather than anxiety.
Other supports that can help alongside ERP
Depending on your situation, treatment may also include:
OCD-informed CBT tools (to spot thinking traps without turning insight into rumination)
Coordination with a prescriber when medication is appropriate
Partner involvement with clear boundaries (supporting you without feeding reassurance loops)
How to deal with relationship OCD day to day
If you’re searching how to deal with relationship OCD, you’re probably looking for practical steps you can try right away. The goal is to shift from trying to wrestle with the content of your doubts, to targeting the cycle that maintains the OCD spiral.
1) Name the urge accurately
When the pull to “figure it out” hits, try labeling it:
“This is an ROCD urge.”
“This is a checking/reassurance urge.”
“My brain is asking for certainty.”
2) Replace reassurance with a brief script
Reassurance tends to calm anxiety briefly and strengthen the loop long term. Scripts help you pivot without escalating the debate.
Try:
“I’m noticing the urge to check. I’m not solving this right now.”
“Maybe, maybe not.”
"Uncertainty is uncomfortable. I'm staying with it anyway."
"This is discomfort, not a signal I need to act on."
If involving your partner, a boundary-friendly script can be:
“I’m having an ROCD spike. I’m working on not asking for reassurance. If I seem distant, it’s anxiety—not you.”
3) Delay the compulsion (start small)
Set a short delay:
“I’ll wait 15 minutes before I ask, check, or research.”
Then increase gradually as your tolerance grows.
4) Reduce high-frequency checking channels
Common “high-reward” channels include Googling, forums, quizzes, and repeated relationship conversations designed to secure certainty. Consider specific limits:
no late-night research
no “relationship review” conversations when anxious
one planned check-in time per week (values-based, not anxiety-driven)
5) Choose values-based actions
Instead of acting from certainty, act from values:
show warmth and presence
engage in shared activities
practice honesty with boundaries (without compulsive confessing)
6) Expect a temporary spike when you stop feeding the loop
If you reduce compulsions, anxiety often rises at first. That doesn’t mean you’re doing it wrong. It often means you’ve interrupted a learned pattern. This is also why guided treatment can be so useful.
FAQ
Is relationship OCD real?
Yes. Relationship OCD is a recognized OCD theme where obsessive doubt and compulsions center on relationships. It isn’t “just being unsure.” It’s a cycle that can take up hours, increase distress, and make it hard to trust your experience.
Can ROCD happen in a good relationship?
Yes. OCD often targets what matters most. ROCD can show up even when the relationship is caring, stable, and aligned with your values.
Does reassurance help ROCD?
Reassurance can calm anxiety briefly, but repeated reassurance often strengthens the cycle over time by teaching the brain that doubt is dangerous and must be solved.
What if I’m with the wrong person?
ROCD pushes you to treat uncertainty as an emergency. Treatment helps you step out of compulsive solving so you can make decisions from clarity and values, not panic and rituals.
Next steps: getting support
If ROCD is taking up time, creating distress, or impacting your relationship, effective treatment is available. You don’t have to solve every doubt to move forward—you can learn new ways to respond to uncertainty and regain space in your mind and your relationship, and our team is ready to help.
Gofman Therapy & Consulting · Westport, CT
Ready to Stop the ROCD Loop?
You don’t have to resolve every doubt before moving forward. We offer a free 15-minute consultation so you can ask questions and get a sense of whether we’re the right fit.
Book Your Free Consultation →In-person in Westport, CT · Virtual across Connecticut & Virginia
David Gofman, LPC, is a therapist at Gofman Therapy and Consulting in Westport, CT. He specializes in ERP for OCD and anxiety disorders, Pain Reprocessing Therapy for chronic pain, and works with teens, young adults, and young professionals in-person and virtually across Connecticut and Virginia.